An end‑to‑end discovery engine, built for translation.
Three operational layers — computational, experimental, and translational — held together by one biological data graph. Programs move forward continuously, not in monthly handovers.
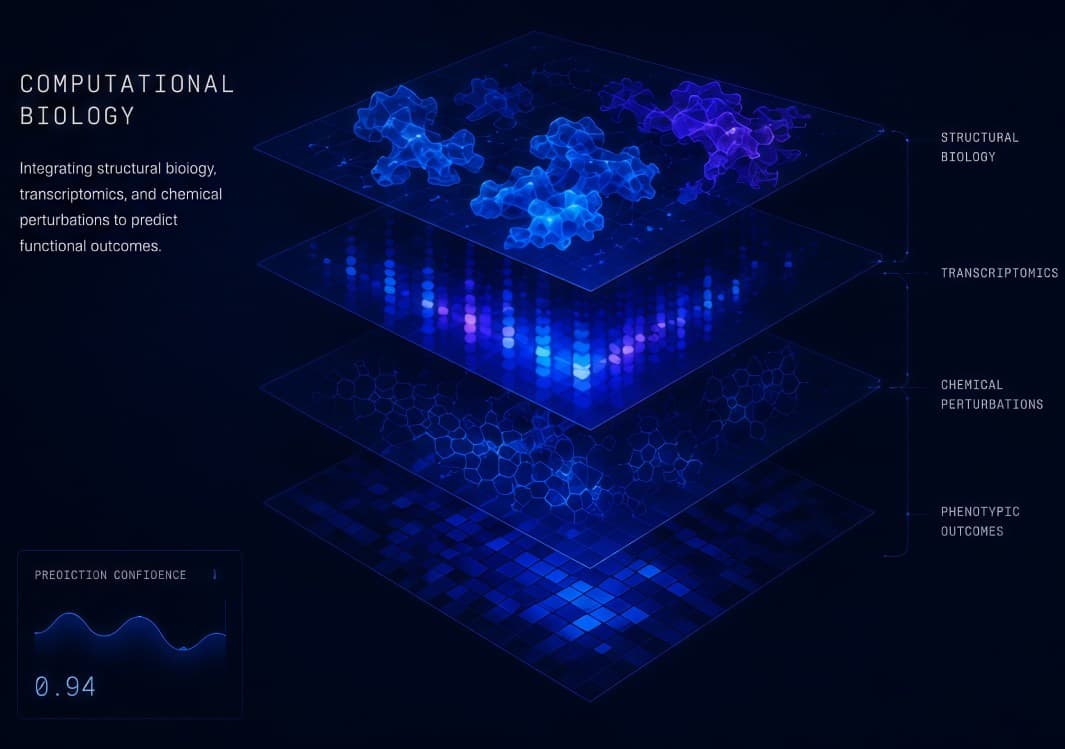
A foundation model trained on 1.2B annotated biological sequences predicts protein–compound interactions in silico — surfacing leads weeks ahead of physical assay.
Unlike vendor screening libraries, our graph is built from first‑principles biology: structural data, longitudinal patient cohorts, organoid readouts, and over a decade of curated literature. It updates nightly with every wet‑lab result that returns from the floor.
- /01 Multi-modal target identification across genomics, transcriptomics and proteomics.
- /02 Generative chemistry proposing 10⁵ optimisable analogues per scaffold, ranked for potency, ADMET, and synthesisability.
- /03 Active-learning loop selects the next 1,000 compounds the wet lab should run each week.
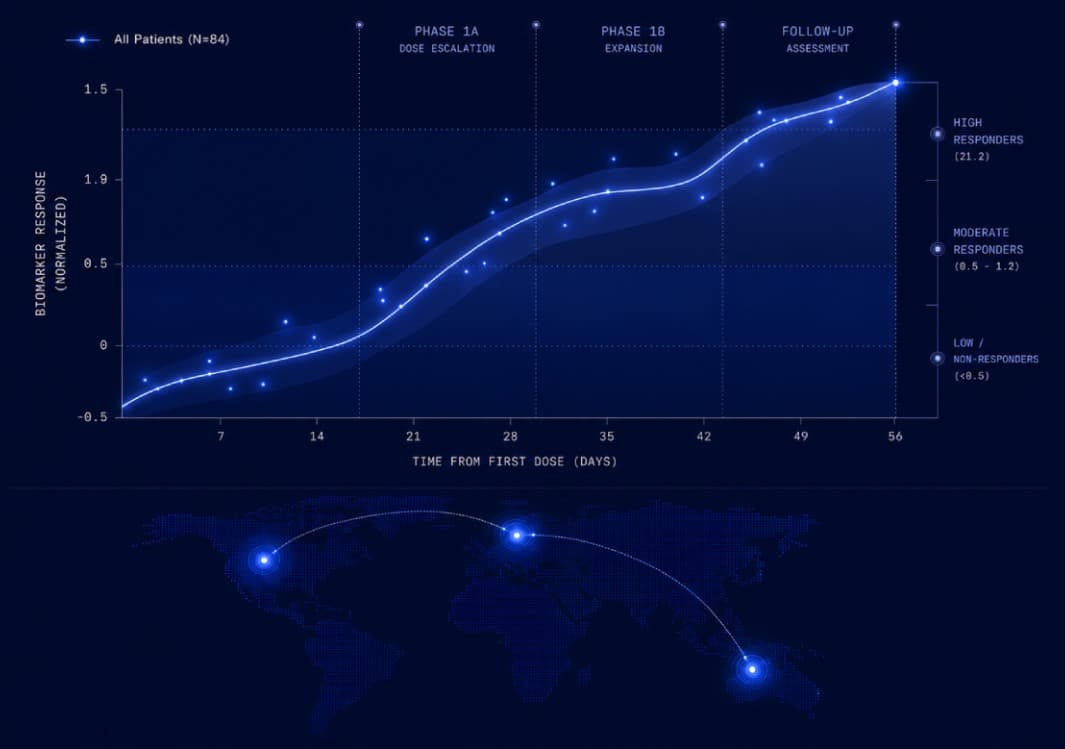
A biomarker‑led clinical team carries promising candidates through IND‑enabling studies and Phase 1 in partnership with academic medical centers across three continents.
Translational biomarkers are designed in alongside discovery, not bolted on at IND. Patient stratification hypotheses are pressure-tested against prospective cohorts before the first dose. Partners get a ready-to-run Phase 1 protocol, not a candidate molecule on a shelf.
- /01 Prospective biomarker design integrated from program initiation.
- /02 DMPK, tox, and CMC delivered via validated CRO network and internal preclinical lab.
- /03 Investigator network across Karolinska, Memorial Sloan Kettering, and INSERM.
A program, end to end.
A typical engagement runs from target nomination through Phase 1 readout in 26–32 months — with continuous data sharing, no quarterly reveals.
Target nomination
Patient multi-omics analysis to identify and validate druggable targets.
Lead generation
Generative chemistry, virtual screen, in-silico ranking.
Wet-lab validation
Robotic synthesis and patient organoid assays.
IND-enabling
DMPK, tox, CMC, GLP packages and biomarker design.
Phase 1
Investigator network, biomarker-led patient stratification.